|
| A cupcake rendition of an OCT showing a macular hole |
What is a macular hole?
To describe a macular hole and how it forms, we need to first discuss the anatomy of the eye. Check out this video for a concise overview of the structures of the eye (it's less than a minute long).
 |
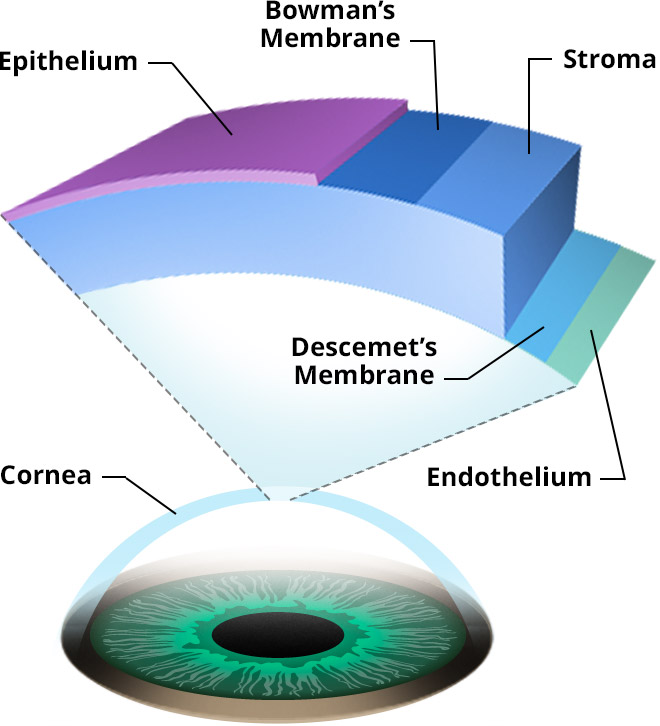
The anatomy of the eye
Image: ASRS
|
Other than the vitreous traction described above, there are some additional causes of macular holes including trauma, high amounts of nearsightedness, diabetic eye disease, and epiretinal membranes (aka macular pucker).
Since they are most often related to aging processes, macular holes are more common in people over 60 years of age. They are also more common in females than males (1).
 |
| A visual of the vitreous detaching from the retina (posterior vitreous detachment, or PVD) Image: Eye |
What are the symptoms of a macular hole?
The macula is the part of the retina that is responsible for your central, sharpest vision. So a macular hole can cause blurred or distorted central vision. You may also notice a dark spot in your central vision.
How is a macular hole diagnosed?
A macular hole is found by your optometrist or ophthalmologist during a dilated eye exam. Fundus photography, as seen below, can be used to document the appearance of the hole, using filters to make the hole more apparent.
 |
| Fundus photo of a patient with a macular hole |
 |
| OCT scan of the above photographed macular hole |
How do you treat macular holes?
Though some small macular holes are left to resolve and seal on their own, many require treatment. The most common way to treat a macular hole is with a procedure called a vitrectomy. That's when a retinal surgeon removes the gel sack in the eye and replaces it with a gas/air bubble. Removing the vitreous relieves the pulling (traction) on the retina, and the bubble puts pressure on the edges of the hole, helping to bridge and seal the hole. In some cases, the inner limiting membrane of the retina is also peeled (jury is still out on whether this is required to achieve the best results in small holes). Most surgeons will advise patients to maintain a face-down position for a few days after surgery, sometimes even as long as 2 weeks (jury is still out on whether this is necessary for small and medium holes). The success rate for this procedure is very high, with estimates ranging between 85 and 100% (2). Cataracts are common following vitrectomy, so some surgeons may opt to remove the lens at the same time as doing the vitrectomy.
Another potential treatment in cases of small or medium holes with traction is injection of ocriplasmin (Jetrea®) into the eye. This drug degrades the adhesion molecules (specifically fibronectin and laminin) at the interface of the vitreous and retina, helping to relieve traction on the retina. With a success rate of 35-40%, ocriplasmin is significantly less successful in achieving closure of macular holes when compared to vitrectomy, especially for medium sized holes (3). It is also less cost-effective in many health systems.
If you've had a macular hole in one eye, you have an increased risk of getting one in the other eye. Estimates vary, but you are looking at a 5-15% chance over 5 years (4, 5). So keep seeing your optometrist for routine eye exams!
CliffsNotes: A macular hole is a hole in the part of the retina called the macula, and it most often occurs as a result of aging processes within the eye. Most cases are treated with a surgical procedure called vitrectomy.
Additional recommended resources: